Any further thoughts on this subject?
From my research, multipiece LF1 traditionally maxes out below 1 cm. Anything 1 cm or more requires SARPE. I haven't talked to Gunson about this though to see his opinion. Has anyone asked him?
SARPE can relapse in part because a lot of the expansion can actually be dental (not from bone). I need 8 mm expansion and Caminiti said he wanted to do SARPE out to 1.1 or 1.2 cm to ensure we have enough expansion even after some anticipated relapse. It needs to be overexpanded to plan for this.
He said a multipiece LF1 would not be viable for me as if we did it for 8-9 mm, the relapse would bring us down to 6 mm or so and then I'm still in crossbite.
I am confused about the widening midface/zygos effect people are claiming from SARPE.
How is a SARPE performed? Are there multiple techniques?
I see this diagram which shows a split just down the middle. This would definitely widen the cheekbones/midface in a favorable way:
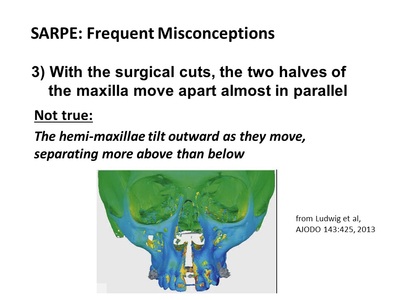
However, I was always under the impression THIS is how SARPE works:

This approach will not in any way widen the cheekbones as you are just basically doing a multipiece LF1 gradually over time. The surgical approach is summarized here, using a bone borne expander:
https://www2.aofoundation.org/wps/portal/surgerymobile?contentUrl=/srg/95b/05-RedFix/P370-SurgAssRapPalExp/05_Expansion.jsp&soloState=precomp&title=&Language=enThis article seems quite thorough on the subject but I'm still not understanding how it can or can't affect the zygos.
http://www.toportho.org/think-pieces/sarpe-a-frequently-misunderstood-surgical-procedureFrom what I understand reading it, the technique implemented in the green CT scan above where the whole midface is widened is the OLD way of doing it that no one does anymore, because it's highly risky and has led to terrible complications when the entire skull fractures from the strain. They say a SARPE is basically exactly the same as a multipiece LF1 in the cuts, except the "down fracture" is more complete in a multipiece LF1. That's it.
So I don't think modern SARPE should provide any benefit to the zygos at all.
The quote most relevant to me is:
Myth: SARPE is needed as the first phase of surgical technique when skeletal transverse and a-p / vertical change are desired.
Why would you do that? In theory, so that in a second surgical phase the maxilla can be repositioned in one piece and the transverse expansion will be more stable.
The problem with that concept is that results with one-phase segmental osteotomy for transverse changes and a-p / vertical repositioning at the same time are remarkably similar to the results with two-phase surgery. At present, there is a divide between surgeons in the northeastern US and eastern Canada, many of whom advocate two-phase treatment for three-dimensional problems, and those in the rest of the US and Canada, who usually manage problems in all three dimensions with a single surgery. The two-phase treatment has greater morbidity, cost, and difficulty in a repeat of the bone cuts that were done in the first procedure. It is hard to justify that if you can get the same results with a single surgery, and orthodontists should be sensitive to this point (3,4).
The bottom line: at present, SARPE offers a slight advantage to the patient in stability and surgical morbidity when only transverse changes from maxillary surgery are needed, and a significant disadvantage when three-dimensional changes are needed. It is indicated only when transverse expansion is all the patient needs.
So maybe I don't need a SARPE at all. I just need someone capable of juggling 2-3 fragments simultaneously and getting it all done at once.

